Drug Rehab in Austin, TX: What to Look For in a Residential Program (2026 Guide)

If you’re reading this, something has already happened. Maybe it’s your own bottom. Maybe it’s a phone call about your son, your husband, your brother. Either way, you’ve started doing the research nobody wants to do, looking for a drug rehab in Austin, Texas, and trying to figure out which one is actually going to work.
This guide is written for that moment. It won’t sell you on a particular facility. It will tell you what genuinely matters when you’re choosing a residential program in the Austin area, what the red flags look like, and what to ask on the first phone call so you don’t waste 30 days and tens of thousands of dollars on a program that was never going to fit.
If you or someone you love is in immediate crisis, call SAMHSA’s National Helpline at 1-800-662-HELP (4357). It is free, confidential, and runs 24/7. For overdose or medical emergencies, call 911.
The state of addiction in Austin in 2026
The need for solid treatment in Travis County is not abstract. According to the Travis County Medical Examiner’s Office, 486 accidental drug deaths occurred locally in 2023, with 279 fentanyl-related deaths that year. The numbers have since started moving in the right direction. Accidental drug deaths fell to 380 in 2024 and to roughly 301 in 2025, with fentanyl deaths dropping about 60% over the same period, as KUT Austin reported on the latest county medical examiner data. Local leaders attribute the decline to expanded access to Narcan, harm-reduction programs, and increased treatment infrastructure.
That improvement is real, but the problem is not solved. Drug overdoses remain the leading cause of accidental death in Travis County, ahead of falls and car accidents. While Narcan keeps people alive in the moment, it doesn’t treat addiction. Treatment does.
The good news: Austin has more credible residential treatment options than it did even three years ago. The bad news: more programs look credible from the outside and aren’t. Here’s how to tell the difference.
Inpatient, outpatient, residential: what’s the actual difference?
These terms get used loosely, and the looseness costs people money and time. The clean version:
Detox is the medical stabilization that happens in the first few days, usually under 24-hour clinical supervision. It is not addiction treatment. It is a treatment for withdrawal. Most people who need it should not skip it, and most people who only do it relapse quickly.
Inpatient or hospital-based treatment is short-term, medically intensive, and typically attached to a hospital or psychiatric facility. It’s for people in acute crisis or with serious co-occurring medical or psychiatric issues. Stays are often 5 to 14 days.
Residential treatment is what most people picture when they say “rehab.” You live at the facility for 30, 60, or 90 days, sometimes longer. The clinical model varies enormously between programs. A good residential program runs a structured daily schedule that combines individual therapy, group work, and experiential or skill-building activity. You can see what that looks like in practice on our program page, which lays out a full day on the ranch.
Partial hospitalization (PHP) and intensive outpatient (IOP) are step-downs. You sleep at home or in sober living and attend programming 3 to 5 days a week. Useful as a transition, rarely strong enough on their own for someone with a serious substance use disorder.
Outpatient is once-a-week therapy. It works for some people. For most people with a recent residential-level problem, it’s the equivalent of trying to put out a house fire with a garden hose.
For someone in early recovery from a serious addiction, the research and the field’s consensus are consistent: residential, followed by structured step-down care, followed by sober living, is the model that gives people the best shot at lasting recovery. Cutting any of those steps usually shortens the recovery.

7 things to look for in an Austin residential rehab
1. A clinical model you can describe in one sentence
If you ask a facility what their treatment philosophy is and the answer is a list of buzzwords (evidence-based, holistic, individualized, trauma-informed, dual-diagnosis), slow down. Every program in America says this. The question is what specifically do you do every day, and why?
Strong programs have an actual answer. Some are 12-step focused. Some use the Matrix Model or CBT-heavy curricula. Some integrate experiential modalities like equine therapy, therapeutic farming, or wilderness work. Some are explicitly faith-based. None of these is right for everyone, but a program that can clearly explain its model is a program that has one. A useful test: ask to see their day-by-day programming and compare what they describe to what shows up on the schedule.
2. The right length of stay
Decades of research point to the same conclusion. The National Institute on Drug Abuse’s Principles of Drug Addiction Treatment states plainly: “Generally, for residential or outpatient treatment, participation for less than 90 days is of limited effectiveness, and treatment lasting significantly longer is recommended for maintaining positive outcomes.”
A 28-day program can be a fine start. It is rarely a complete treatment. If a facility is selling you 30 days and discharge, ask what their plan is for days 31 through 90, because the research is clear that long-term residential care produces materially better outcomes than 30-day stays. If the answer is vague or relies entirely on outpatient handoff, that’s a yellow flag.
3. Real clinical staff with real licenses
Ask, by name, who the clinical director is. Ask what their credentials are (LCSW, LPC, LCDC, LMFT, psychologist). Ask the staff-to-client ratio. Ask how many of the people running groups are themselves licensed clinicians versus peer recovery coaches. Both have value, but a program with no licensed clinicians on staff is not a treatment program. It’s a sober living house with a marketing budget.
4. Medical and psychiatric capacity
A serious percentage of people entering residential treatment also have an untreated mental health condition like depression, anxiety, PTSD, or bipolar disorder. Programs that don’t have a psychiatrist (or contracted access to one), can’t manage psychiatric medications, and can’t treat the underlying mental health condition are going to lose those people. Ask: is there a psychiatrist on staff or under contract? How often do clients see them?
5. A specific aftercare plan
Ask, before you admit: what does the discharge plan look like? If the answer is “we’ll figure that out at the end,” walk away. A good program is thinking about aftercare from intake day one, including sober living, IOP step-down, peer support, family work, and continuation of medication-assisted treatment where applicable. The 90 days after discharge are statistically the highest-risk period for relapse. The program should treat them that way.
6. Family involvement that’s more than a brochure
Addiction is a family system problem. Programs that work to engage the family through education, family therapy sessions, structured visiting, and support for codependent or enabling patterns generally see better outcomes. Ask: How do you involve family during treatment? If the answer is “we have a weekly call,” that’s a thin offering.
7. The setting matches the person
This is the part most people are underweight. A 22-year-old male whose addiction has wrapped itself around a city nightlife scene generally does not get well in a hotel-style facility a few miles from the bars he used to drink at. Distance from the using environment, the structure of the daily schedule, the type of work or experiential activity built into the day, and the gender composition of the program all matter more than glossy amenities. A ranch or farm-based setting in particular gives men in early recovery something most urban facilities can’t replicate: physical labor, time in nature, animals, and a daily structure that’s mechanically incompatible with the patterns that fed the addiction.
What it costs, and what insurance actually covers
Residential treatment in Texas typically runs $15,000 to $45,000 for a 30-day program, with longer or higher-amenity programs going higher. Most reputable facilities work with major commercial insurance (Aetna, Blue Cross Blue Shield, Cigna, United, and others) for some portion of the stay. Coverage varies dramatically by plan and by medical necessity criteria.
A few things to know:
- In-network vs. out-of-network makes a large difference. Always ask whether the facility is in-network with your plan before admission.
- Verification of benefits should be free and should happen before you sign anything. A facility that pressures you to admit before benefits are verified is a facility that’s planning to bill you, not your insurance.
- Cash-pay rates are sometimes negotiable, especially for longer stays.
- Texas Medicaid does not generally cover private residential treatment for adults, but state-funded options exist through public referral channels.
- Beware “free rehab” advertising. There are legitimate state-funded options, but most “free” advertising online is lead-generation that sells your contact info to whoever bids highest. Use FindTreatment.gov, the federal treatment locator, instead.
Red flags to walk away from
Twenty years in the field have produced a fairly stable list:
- The intake call is run by a salesperson, not a clinician. Admissions people are normal. Aggressive sales scripts are not.
- The program promises a specific outcome. No one can ethically promise sobriety. The honest version is: “We can give you the best shot we know how to give.”
- They pressure you to admit today. Urgency tactics (“we have one bed left this afternoon”) are sales tactics.
- They won’t say who their clinical director is, or the answer is vague. Run.
- They offer to fly you in for free. This is sometimes legitimate, often a sign of an insurance-fraud-adjacent operation that needs to fill beds.
- They won’t show you the facility on a video call before admission. Any real program will do this.
- The website is full of stock photography of unrelated people. Honest programs show their actual building, their actual staff, and their actual clients (with permission).
- They badmouth other facilities. Healthy programs don’t need to.
Questions to ask on your first call
Print this list. Take notes on the answers.
- What is your clinical model in one sentence?
- Who is your clinical director, and what are their credentials?
- What’s your staff-to-client ratio? How many licensed clinicians are on staff?
- Is there a psychiatrist on staff or under contract?
- What does a typical day look like?
- What’s the average length of stay? What does your aftercare planning look like?
- How do you involve family during treatment?
- What insurance do you take? Are you in-network with my plan?
- Can I do a video tour of the facility before admitting?
- Can I speak with an alumnus of your program?
The last one is the most telling. Programs that produce real recovery have alumni who will pick up the phone.
What recovery looks like after 30 days
The hardest thing for families to hear is that a successful 30-day stay is the beginning, not the end. The data is unambiguous: people who do residential treatment and immediately return to the environment they used in have very high relapse rates. People who step down through structured aftercare (extended residential, sober living, IOP, peer support, ongoing therapy) do dramatically better at the one-year and five-year marks.
That doesn’t mean treatment has to be 90 days residential. It means treatment has to continue after the residential piece in some structured form. Anyone telling you otherwise is selling you a product, not a recovery.
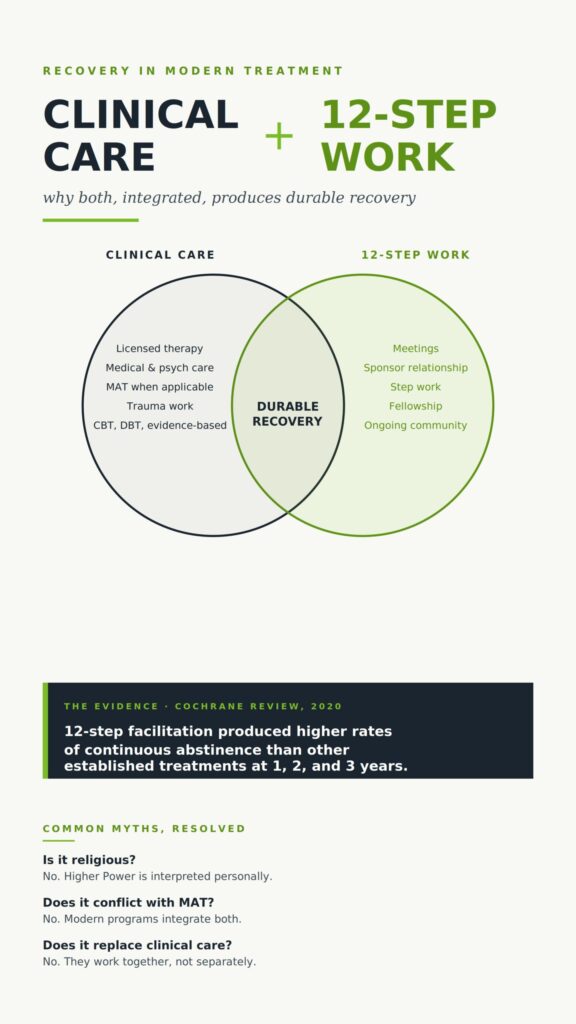
Where Ranch House Recovery fits
Ranch House Recovery is a residential addiction treatment program for men in the Austin area, built on a working ranch outside the city. The model is regenerative: therapeutic farming, animal-assisted work, the 12 steps, evidence-based clinical care, and a daily structure that physically and psychologically separates men from the using environment. Length of stay is built around what the research actually supports, not around what a 28-day insurance benefit will pay for. If you want a sense of how that model came together and the thinking behind it before you call, our philosophy is the most honest two-minute read on the site.
The bottom line
Choosing a drug rehab in Austin is not a marketing problem. It’s a fit problem. The best program in the country is the wrong program if it’s not the right fit for the person. The questions above won’t tell you which facility is “the best.” They’ll tell you which ones are real, which ones are honest, and which ones are built to do the work.
If you’re ready to talk about whether Ranch House Recovery is the right fit, you can reach admissions here. If we’re not the right fit, we’ll tell you, and we’ll try to help you find one that is. That’s how this is supposed to work.